Inequalities in the Dementia Pathway: Lessons from the Alzheimer’s Society Conference
Insights from the 2025 Alzheimer’s Society Conference on dementia care inequalities across policy, services, communities and families in the UK.
For me, dementia is not abstract policy — it is close, lived, and felt, shaping the way I hear stories, weigh evidence, and frame change. Attending the Alzheimer’s Society Annual Conference 2025 last week sharpened this lens: a stage where politics and practice collided, exposing both promise and tension.
The panel made painfully clear where the structural inequities lie: music therapy and community programmes left at the discretion of local NHS Trusts, never guaranteed, never mandated. Good practice exists — but only if you happen to live in the right postcode, under the right trust, with the right will to implement it.
Richard’s story cut through the jargon. His mother’s fractured wrist was treated, but her diabetes neglected — despite clear national case law that should have made her care a macro-level responsibility. A broken system treating body parts in silos, rather than people as whole.
This is political inequity in its most concrete form: absence of national mandate, fragmentation between specialties, invisibility of outcomes that cannot be easily measured. What is not codified into policy remains optional, and what remains optional becomes unequal.
And then came the Minister Stephen Kinnock spoke not just as a politician, but as a son who had seen dementia close-up. His 10-Year Health Plan carried the promise of three seismic shifts: hospital to community, analogue to digital, sickness to prevention. Within it, dementia was named as a national priority, framed not as a side-note but as a core test of the system’s fairness. He pledged a modern service framework for frailty and dementia, designed to reduce unwarranted variation, and anchored it with tangible commitments: £150 million for the Dame Barbara Windsor Dementia Goals Programme, £11 million for digital innovation, new carer pathways, even an independent commission to push adult social care out of the political football it has long been.
And yet, as inspiring as the tone was, the tension lingers. The gap between rhetoric and reality is exactly where inequity grows. If frameworks are to matter, they must move from promise to mandate. If funding is to mean something, it must embed practice so that Trust-level discretion no longer decides who benefits. And if carers are to be recognised, their voices must shape not only apps and allowances but the way the system itself is designed.
This is where the political and the practical must meet: not in abstract vision statements, but in closing the very inequities the panel laid bare. The layers of those inequities became clearer as the conference unfolded.
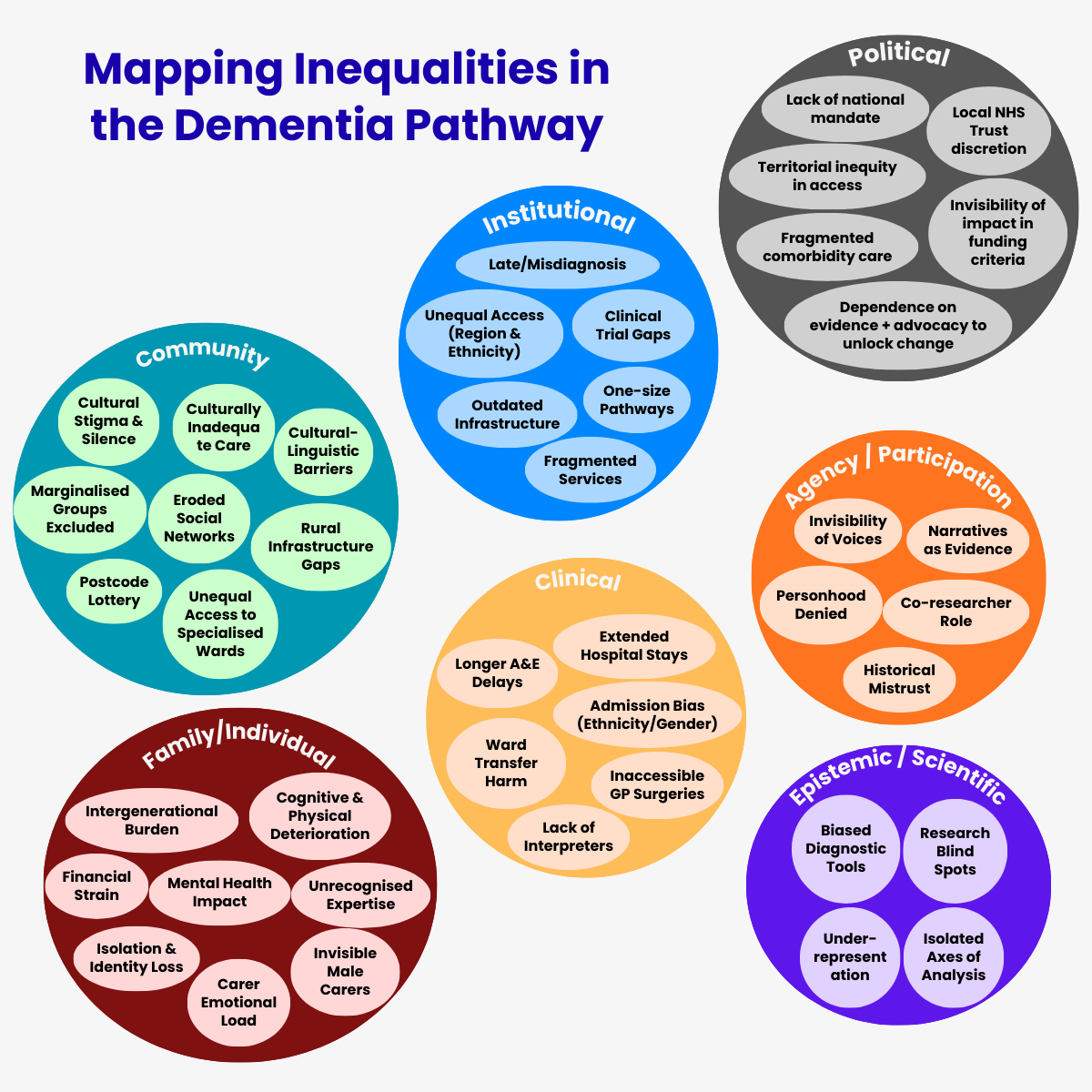
Inequalities map
The opening of the conference made those inequities visible from the start. Listening back, what stays with me is not only the statistics, but the human weight behind them.
The first layer is institutional: a system that should diagnose and guide, but too often misdiagnoses, delays, or fragments. A fax machine still in use in 2021; a GP who dismisses early symptoms as “stress”; a postcode that determines your chance of being seen. These are not isolated anecdotes but symptoms of a structure that is outdated and uneven. The picture that emerges is one of late and inconsistent diagnosis, unequal access, outdated infrastructure, fragmented services, and one-size-fits-all pathways that fail to reflect the diversity of real lives.
Then comes the community level — the quieter terrain where stigma and silence do their damage. In ethnically diverse communities, dementia is still spoken of in hushed tones, or not spoken of at all. Families do not know where to turn, and when they do, they face the “postcode lottery” that makes geography a determinant of dignity. Rural and coastal areas lack even basic provision; carers who can speak the right language are almost impossible to find; social networks wither under the pressure. These are the phrases that linger: cultural stigma, lack of awareness, postcode lottery, rural gaps, inadequate cultural competence, eroded networks. They are the invisible threads that isolate people long before the system itself enters the room.
And then, most viscerally, the individual and family level. Here inequity is not abstract but lived daily: the son who shoulders the burden when his parent deteriorates; the worker forced out of employment; the carer whose mental health, marriage, and sense of self slowly unravel. The word that repeats itself is invisibility. Carers described as “aggressive” rather than recognised as experts; families carrying a load that institutions neither see nor acknowledge. Behind the statistics lie intergenerational burdens, financial strain, isolation, the emotional toll of caring, and expertise that remains unrecognised.
What emerges across these three layers is not a set of isolated problems, but a pattern. Inequities recur: misdiagnosis, geography as destiny, cultural blind spots, and the quiet collapse of carers under invisible weight. And yet, amidst the gaps, there are seeds of hope: £2 million for research into inequalities, new doctoral centres, nurses trained to diversify trials, blood biomarkers that could transform diagnosis, and policy frameworks beginning to take shape across the nations.
The story here is not one of despair, but of contrast. Inequalities laid bare at institutional, community, and family levels — and, alongside them, the first signs of a response. The challenge is not that we cannot name the categories, but that we still struggle to act on them with the urgency they demand.
But inequity is not confined to services alone; it also hides in the evidence itself — in the frameworks and tools that shape how dementia is seen, diagnosed, and defined.
As Dr Ben Hicks, Principal Research Fellow at Nottingham University and Programme Manager for DETERMIND, reminded us, early is not always timely. Two years can pass between first noticing symptoms and receiving a diagnosis, and those two years are distributed unevenly: poorer families wait longer; ethnic minorities face tests never designed for them; those with more education can mask decline until the moment of collapse. Even the meaning of “timely” diverges: what feels urgent for a carer may not feel right for the person themselves. And layered onto this was the pandemic — memory services suspended, diagnoses postponed, lives placed on hold. The patterns are familiar: biased tools, under-representation, structural delays, rural transport gaps, and a fractured sense of timeliness.
STRiDE, presented by Adelina Comas-Herrera — Director of the Global Observatory of Long-Term Care at the London School of Economics and co-lead of the Strengthening Responses to Dementia in Developing Countries project — takes this further, showing how inequity accumulates when life is seen through a single lens at a time. The literature speaks of ethnicity or poverty or gender, but rarely of their intersections. And so lives like Chris’s slip through the cracks. Three months after diagnosis he lost his job, and ever since has fought for recognition — fighting stigma from professionals who addressed his companion rather than him, and fighting systems that saw his dementia first and his personhood last. The labels here read: loss of rights, institutional stigma, invisibility of voice, and absence of intersectional frameworks.
Yet both projects offered glimpses of another path. Longitudinal cohorts that include carers as well as patients. Doctoral work that explores coping strategies as a lever for earlier diagnosis. Tools designed not only to confirm decline but to deliver hope. Narratives treated as evidence in their own right. People with dementia and carers editing, correcting, co-authoring what will be said about them. The principle is simple but radical: nothing about us without us.
Together, they add two further layers to the inequalities map: the epistemic level, where inequity is produced by methods, instruments, and frameworks that fail to capture lived complexity; and the agency level, where inequity is either undone — or entrenched — depending on whether voices are silenced or invited into co-creation. They remind us that inequality is not only about services failing to reach people; it is also about knowledge failing to see them.
But even within this uneven landscape, some stories showed what is possible when priorities shift.
Three lessons in tackling inequalities
Success rarely looks like a miracle intervention. It looks instead like a quiet re-ordering of priorities — one decision, one relationship, one method of care at a time.
The Northern Care Alliance showed that success can be as simple — and as radical — as not moving people. In a system obsessed with throughput, they dared to remove beds and turn them into activity spaces. They created dementia units where patients were admitted directly from A&E and never shuffled again until discharge. The results spoke for themselves: families reported better experiences, patients left six to eight days earlier, and the trust saved thousands of bed days. What really worked here wasn’t the “squiggly charts,” as the director put it, but the courage to let data point back to people — to ask not only how long patients stayed, but how they were treated in between.
The Bristol Dementia Wellbeing Service offered a different kind of success — one rooted in trust. Their “recipe for change” was not a metaphor but a method. They worked slowly, deliberately, with communities who had every reason to mistrust the system: Polish women’s groups, Somali carers, Chinese men carrying their isolation in silence. They did not parachute in with ready-made solutions; they built relationships, listened, made films in people’s own languages, and returned again and again. The payoff was ownership: communities running their own groups, holding services to account, shifting from fear to knowledge. The value lay not only in reduced stigma or increased referrals, but in the ripple effect — the sense that leadership and advocacy could grow from within.
Nordoff Robbins reminded us that equity does not always arrive as policy. Sometimes it comes through music. They reframed music therapy from “nice to have” into an essential care pathway. In practice, that meant moments of breakthrough: a woman once silent singing “I, I, I” in time with her therapist’s guitar; a man of Caribbean heritage, withdrawn in daily care, suddenly leading a call-and-response gospel song that drew others into his rhythm. What mattered was not performance, but recognition — music amplifying identity and agency when words and conventional care fell short. It reduced agitation, lowered reliance on medication, supported staff morale, and gave families a new language of connection that bypassed decline.
Across these three cases, the common success lies in seeing what is usually unseen: the hidden harm of ward moves, the silent carers who never ask for help, the cultural resonance of a song that restores dignity. Each story is a reminder that tackling health inequalities is not about scaling the perfect model. It is about noticing, adjusting, and staying with the work long enough for trust, creativity, or music to do their quiet, radical work.
Knowledge transfer
By the end of the conference, the conversation felt like looking into a hall of mirrors. Diabetes, cardiovascular disease, Parkinson’s — different conditions, yet each reflecting the same distortion: inequities falling hardest on women, on minority communities, on those without resources or representation. And still, the mirrors offered something else: lessons, hints at what could be done differently.
Ruth Chauhan’s framing was sharp: diversity is a fact, inclusion is an act. She showed how diabetes and heart checks could become less stigmatising gateways for communities who avoid the word “dementia”. A simple shift — talking about healthy ageing, reducing risks — could open doors that stigma had kept firmly shut. That is knowledge transfer in practice: borrowing language, reframing entry points, recognising that one visit can serve multiple purposes and save people from a maze of disconnected silos.
From Diabetes UK came another insight: optimism matters. It is not enough to highlight disparities; professionals and politicians need evidence of improvement to believe change is possible. Embedding community voices in research funding, financing local NGOs so they are not asked to contribute for free, creating one-stop shops to reduce barriers — these are transferable mechanisms. The inequities may be familiar, but so are the levers to reduce them.
Cardiovascular disease brought the gender lens into sharper focus. Women misdiagnosed, under-treated, invisible in the data — how different is that from what we suspect, but have not yet fully measured, in dementia? The strategy here was clear: demand disaggregated data, design sex-specific protocols, and use the shock of hard statistics to drive awareness. Again, a ready-made template waiting to be applied.
And Parkinson’s UK reminded us that change often begins where exclusion is deepest. They started with race and ethnicity, investing in trust and networks before ever speaking of research. They changed internal processes — funding calls, communications, partnerships — so that inclusion was not left to goodwill but became structural. That too is transferable: in dementia, we can begin where the silence is loudest.
These sessions did not simply describe problems; they handed over tools. They were not about reinventing the wheel, but about learning from wheels already in motion. For me, that is the catalytic role of knowledge transfer: to see dementia not as an isolated field, but as part of a wider pattern of health inequity — and to dare to borrow what works elsewhere.
Reflection
Walking away from the conference, what stays with me is not just the detail of policies or programmes, but the reminder that change is always systemic. Inequalities are never one problem in one place; they are patterns that repeat until we choose to disrupt them. For me, this is where programme management and transformation truly matter — not as checklists or delivery plans, but as the discipline of aligning vision with practice, voices with power, and evidence with action. The task ahead is not to add more reports to the shelf, but to keep building structures that make equity the default rather than the exception.
The closing words of Dr Kamel Hothi OBE, Ambassador of Alzheimer’s Society, still echo: “I do believe everybody here has accountability and ownership to make a change… let’s be the change you want to see in the world”. It was a reminder that transformation is never abstract; it begins with us, and with the choices we make about the systems we shape and the people we serve.